Understanding Pain After Fracture: Why It Happens and Why It Sometimes Persists
Fractures are among the most common injuries worldwide, and although most people heal well, a significant number continue to experience pain long after the bone has united. With global aging and rising osteoporosis, the number of fractures—and complications such as delayed healing or nonunion—is expected to grow. For many patients, the ongoing pain becomes more disabling than the injury itself and can severely limit mobility, confidence, and quality of life.
Pain immediately after a fracture is normal and, in many ways, protective. It discourages excessive movement and weight-bearing, preventing further damage. In a healthy recovery, pain gradually eases as the bone stabilizes, weight-bearing improves, and gait becomes more symmetrical again. However, when pain persists longer than three months, it is considered chronic—and this is where therapists often become central to patient recovery.
Why Does Pain Become Chronic?
While many patients improve with time, 13%–90% (depending on the fracture and treatment) develop some form of chronic post-fracture pain. This may include:
- Pain with loading or exercise
- Sensitivity to light touch (allodynia)
- Heat or cold hypersensitivity
- Ongoing pain despite radiographic healing
Both nonmodifiable (age, sex, injury severity) and modifiable factors (smoking, obesity, delayed surgery, stress, anxiety, or depression) influence who develops persistent pain. Psychosocial health is particularly important—patients with high fear, anxiety, or catastrophizing have a much higher risk of long-term pain.
A small portion of patients develop Complex Regional Pain Syndrome (CRPS), where the nervous system over-reacts to injury. These patients experience swelling, burning pain, temperature or colour changes, and movement difficulties that can severely limit function.
How the Nervous System Drives Fracture Pain
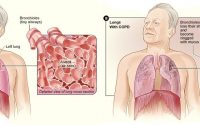
Bone is highly innervated. Nerve endings densely occupy the periosteum (the bone’s outer layer), making fractures extremely painful. After injury, several processes occur:
- Immediate activation of Aδ and C-fibers → sharp and then aching pain
- Inflammation and chemical sensitization → nerves become more reactive, even to light touch
- Peripheral nerve sprouting → nerves grow excessively in the injured area, heightening sensitivity
- Central sensitization → the spinal cord and brain become “wound up,” amplifying pain signals
- Emotional modulation → mood, stress, and trauma influence how pain is interpreted and remembered
Together, these mechanisms explain why pain can continue even after the bone has healed.
Pain Assessment: Clinical and Research Insights
In clinical settings, pain is typically measured using scales such as the Numeric Rating Scale or Visual Analog Scale, but these capture only intensity—not the complexity of chronic pain. More holistic tools such as PROMIS Pain Interference are emerging but are not yet widely adopted.
In research, animal models help scientists study both evoked pain (reaction to touch, heat, or cold) and spontaneous pain (changes in weight-bearing, gait, or guarding behaviours). These models help test new treatments and reduce reliance on opioids.
Medication: Benefits and Problems
Most post-fracture pain is treated with NSAIDs (like ibuprofen) or opioids. NSAIDs reduce inflammation but are sometimes avoided because of concerns about delayed bone healing. This has led to a heavy reliance on opioids—even though they carry risks of dependence and addiction. Today, professional guidelines encourage multimodal pain management, with reduced opioid use and a greater role for non-drug therapies.
What This Means for Therapists
Because fracture pain is not only structural but also neurological and psychosocial, therapists play a crucial role in preventing chronic pain. Key principles include:
- Graded weight-bearing to support bone healing and prevent fear-avoidance
- Gait retraining to restore loading symmetry
- Education to reduce anxiety and catastrophizing
- Monitoring for CRPS red flags
- Movement before medication whenever possible
- Close communication with surgeons and pain teams
By addressing both the nervous system and the musculoskeletal system, therapists can help steer patients away from chronic pain pathways.
Take-Home Message
Fracture pain is more than a broken bone—it’s a complex interaction between biology, biomechanics, inflammation, and the nervous system. Most pain is helpful and temporary, but in some patients it becomes amplified and persistent. With rising fracture rates and increasing awareness of opioid harm, therapists are in a powerful position to guide recovery through education, movement, graded loading, and early recognition of pain sensitization.
Reference:
Nishimura H, Layne J, Yamaura K, Marcucio R, Morioka K, Basbaum AI, Weinrich JA, Bahney CS. A bad break: mechanisms and assessment of acute and chronic pain after bone fracture. Pain. 2025 Nov 1;166(11):e491-505.

Massage Timing Affects Post-exercise Muscle Recovery and Inflammation
Fascia can actively contract and thereby influence musculoskeletal dynamics