Aspects of Fascial Anatomy Relevant to Bodywork
At the 2012 Fascia Research Congress in Vancouver, physiatrist, Dr. Antonio Stecco, and physiotherapist, Julie Ann Day are teaming up to present a full day, post-conference workshop entitled “Fascial Manipulation and its Biomechanical Model”. Furthermore, Dr. Carla Stecco, orthopaedic surgeon and anatomy researcher, is an invited keynote speaker as well as being part of the scientific committee.
The more we know about fascial anatomy, the more our clinical work can be effective. The Stecco family and their collaborators continue to produce new studies about fascia, emphasizing the importance of researching this tissue in depth. Here is some information I gather from their findings.
First, it is important to distinguish between the superficial fascia (SF) and the deep fascia (DF) layers.
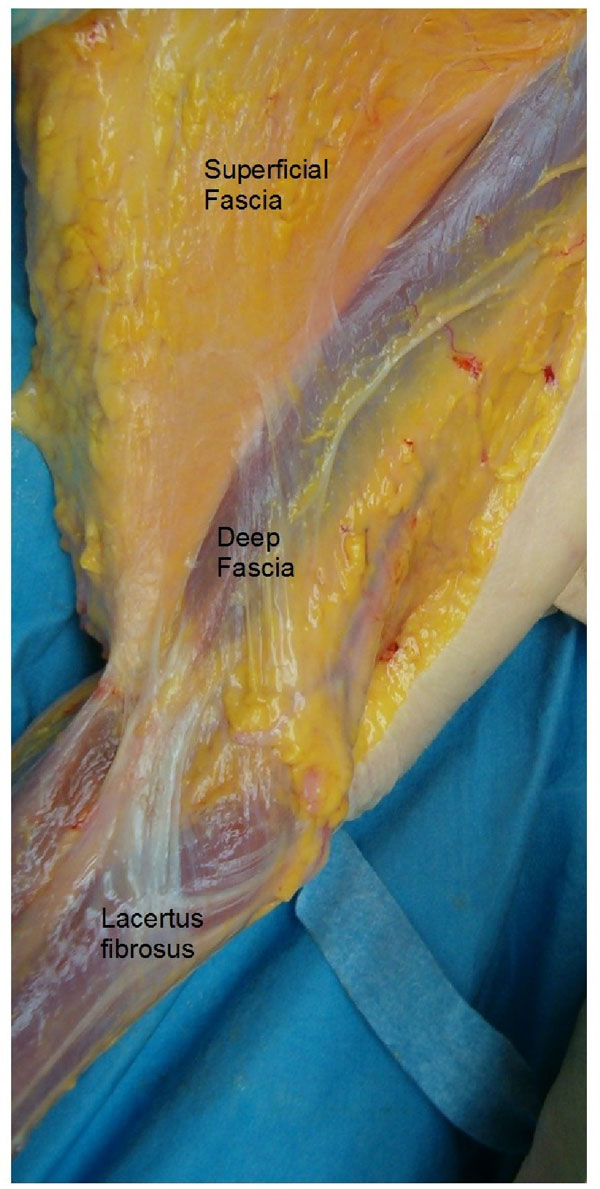
Dissection by Dr. Carla Stecco showing superficial and deep fascia of anterior brachial fascia region. Lacertus fibrosus is highlighted to demonstrate its role as a myofascial expansion between upper arm and lower arm. Image Copyright Dr. Carla Stecco.
This is important because they are distinctly different in terms of structure and function. According to the Stecco studies, the superficial fascia is a membranous layer rich in elastic fibres lying beneath the cutis and within two layers of what is called the “retinacula cutis”. The retinacula cutis layers consist in fibrous septa that extend vertically from the skin to the SF, and somewhat obliquely from the SF layer to the DF; adipose lobules lie between these fibrous septa. In general, the hypodermis layer is involved in the gliding of skin on underlying structures, thermoregulation, metabolic exchange, and the passage of nerves, blood, and lymphatic vessels. Clinically, it is probable that light touch techniques (e.g. lymphatic drainage, superficial massage and others) produce effects within this layer.
The deep fascia lies below the hypodermis, forming a sleeve-like layer, particularly in the limbs, which surrounds muscle groups. This layer is continuous with intermuscular septa, the epimysium (and consequently perimysium and endomysium) and, in some areas, with periosteum. The DF as compared to the SF has a robust, multilayer collagen structure and relatively fewer elastic fibres. It is thought to have a mechanical function of force transmission and, due to the large numbers of embedded mechanoreceptors, a possible proprioceptive role. Clinically, it appears probable that sustained or deep friction techniques are capable of altering tissue consistencies in this layer.
Interestingly, recent studies1,2 have shown that the deep fascia layer in the trunk is quite different, both morphologically and functionally, from that of the limbs. Generally, apart from the thoracolumbar region, the deep fascia of the large superficial muscles (e.g. pectoralis major, latissimus dorsi and trapezius) is thinner (approximately 300 micro meter, 1 micron is a millionth of a meter) because these muscles actually develop within the superficial lamina of the deep fascia, and are not separable from the same. This fascia adheres to these muscles via numerous intramuscular fibrous septa. Many muscular fibres are inserted into both sides of these septa and into the fascia itself, which provides additional insertions for these fibres. In fact, these muscles originate in the embryo as part of the limbs muscles but they then extend towards the midline of the trunk. Migration of limb muscles into the trunk forms an additional myofascial layer with respect to underlying muscular planes. This ensures functional continuity between limbs and trunk, including myofascial connections between the upper and lower limbs, and the two upper limbs. This firm relationship between trunk fascia and muscles allows for fine orientation of the vectorial forces created by the activation of the muscles: different portions of these muscles are activated according to the degree of movement. This modulates the transmission of tension more effectively.
On the contrary, the DF in the limbs is a relatively autonomous structure with respect to the underlying muscular plane. It is a much thicker (0.5 -1.8 mm), with multi-layers of parallel collagen fibre bundles, each layer oriented in a different direction. The difference in direction between one layer and the next has been repeatedly measured to be around 78 degrees. That means that the DF layer can respond to outside stretch quite nicely, with each collagen bundle layer being capable of sliding a little on one another.
In the lower limbs, the DF has significantly fewer elastic fibres as compared to DF in the upper limbs. It is easily separable from the underlying muscles due to the presence of the epimysium, which permits to the muscles to slide independently from the overlying DF. A thin layer of loose connective tissue between DF and epimysium further facilitates sliding. The DF in limbs can perceive contractions of the muscle it surrounds due to myofascial expansions that the muscles extend to the fascia and muscle fibres that insert directly onto its inner surface. We can say that limb fascia is less adaptable than trunk fascia but, being ideal for the transmission of force, it is suited to the function required of our limbs.
The body is a complex system made up of interacting sub-systems. We require interpretative models that simplify the complexity.
Stecco’s biomechanical model3 is an interpretation of one of the body’s sub-systems, namely the fascial system and its focus is on the role of the DF within the musculoskeletal system. It essentially shifts our focus from muscles with origins and tendinous insertions moving bones, to motor units activating groups of muscle fibres united by fascia that bring about movement. It suggests that deep muscular fascia could act as a coordinating component for motor units grouped together into functional units (called Myofascial Units: MFU). Stecco has identified key areas of the deep fascia, called Centres of Coordination, where the tensional forces of each MFU coincide. If the DF in these areas is not sliding, then the MFU will be dysfunctional. The premise is that if manual work can restore gliding to the DF in these key areas then it can influence poor muscle recruitment, myofascial force transmission, faulty movement and pain avoidance patterns.
For example, in RSI (repetitive stress injuries) it is often important to look beyond the local area of strain, questioning our clients carefully about past injuries in order to identify areas that may have never resolved completely in terms of fascial gliding. While deep fascia derivatives (endo, peri, and epimysium) unite the muscle fibres of single MFUs, the myotendinous expansions mentioned above, together with biarticular muscles, form anatomical bridges between adjacent body segments to form myofascial sequences (see photo of lacertus fibrosus as an example) . Therefore, myofascial sequences on each plane essentially unite single MFUs together. Knowledge of myofascial sequences can help us to trace back to the origin of a given dysfunction.
The perception of altered segmental tissue texture and its modification during therapy is a daily experience for most soft tissue therapists.
Trauma and injury can apparently alter fascia but further studies are necessary to clarify what actually changes in pathological conditions. Different authors claim that trauma/injury can alter properties of the extracellular matrix due to neurophysiological influences, with water loss in the tissue influencing collagen fibre bundle formation and orientation. Others implicate changes in fibroblasts with their transformation into myofibroblasts. Reduced gliding between layers of collagen fibre bundles within the deep fascia could result in an alteration of the mechanical properties of the fascia.
Fascia demonstrates viscoelasticity, a material property whereby the deformation (strain) that results from a load (stress) will vary with changes in the rate and amount of loading. Loads within the elastic limits of the tissue will deform it but then it gradually returns to its original resting length after the load is removed. Dr. Antonio Stecco is currently researching the role that hyaluronic acid, one of the components of the extracellular matrix, plays in the gliding and the inflammatory response within fascia. It is likely that a modified viscoelasticity of the extracellular matrix, with subsequent misalignment of the endofascial collagen fibres, will affect the fascia’s capacity to elongate and to adapt to stretch from muscle fibres.
By applying localized friction in an area of palpable rigidity, therapists can create local heat and this may increase certain chemical reactions within tissues such as reduced secretion of inflammatory cytokines. In a recent clinical study4, it was seen that it takes an average of 3.4 minutes of deep friction for a perceptible change to occur in rigid tissues. The redistribution of water from the tissue to the anatomical spaces surrounding the tissue also appears to be involved. This change in viscosity seems to involve an increase in the production of hyaluronic acid, and this acid also has interesting intrinsic anti-inflammatory capacities. Improved drainage of inflammatory mediators and metabolic wastes possibly contribute to the changes we feel under our hands. In addition, by reducing chemical irritation of the various receptors within the tissues our clients can experience a reduction in pain and a renewed freedom in movement.
Hopefully, we will gain a lot more information about all this at the next Fascia Research Congress.
References
1 Stecco A, Masiero S, Macchi V, Stecco C, Porzionato A, De Caro R. The pectoral fascia: anatomical and histological study. Journal of Bodywork and Movement Therapy 2009;13(3):255-261.
2 Stecco A, Macchi V, Masiero S et al. Pectoral and femoral fasciae: common aspects and regional specializations. Surgical and Radiological Anatomy 2009;31: 35-42.
3 Stecco L, Stecco C. Fascial Manipulation: Practical Part. Padova: Piccin; 2009.
4 Borgini E, Stecco A, Day JA, Stecco C, How much time is required to modify a fascial fibrosis? Journal of Bodywork and Movement Therapy 2010; 14(4) 318-325.
About the Author
Julie Day is a physiotherapist originally from Adelaide, and have been living and working in Italy since 1984. She have always used Connective Tissue Massage in her practice and met Luigi Stecco in 1991 in Milan, at a congress about fascia. However, she didn’t get around to do Luigi’s course until 1999. She became a Fascial Manipulation teacher since 2003. She has taught courses and workshops in Italy, Poland, and USA. She is the translator of Fascial Manipulation English editions (2004, 2009). She is also a founding member of Fascial Manipulation Association in Italy. She presented a one day workshop with Dr. Carla Stecco at the 2nd Fascia Congress in Amsterdam.
Exercise reduces musculoskeletal pain—but not because people get stronger

Late Rehabilitation after an Acute Muscle Injury Results in Delayed Recovery
