Rethinking Achilles Tendinopathy Risk in Runners
Achilles tendinopathy is one of the most common overuse injuries seen in runners. It can be persistent, frustrating and difficult to manage because it is rarely caused by a single factor. Training load, tendon capacity, age, previous injury, muscle function and running biomechanics may all contribute to the development of symptoms.
For therapists, one of the major clinical challenges is deciding which factors are truly relevant. Runners are often advised to change their foot strike, reduce pronation or adopt a “better” running style. However, much of this advice has been based on retrospective or cross-sectional studies, where it is difficult to know whether a movement pattern caused the injury or developed as a compensation after the injury.
A recent prospective cohort study provides useful new insight. The study followed a large group of runners and non-runners for one year, measuring baseline running biomechanics, training exposure and later development of medically diagnosed Achilles tendinopathy. Because participants were initially free from Achilles symptoms, the study offers stronger evidence about possible risk and protective factors.
Running volume remains a major risk factor
The clearest clinical message is that weekly running volume matters. Participants who developed Achilles tendinopathy tended to run substantially more than those who remained uninjured. In the statistical model, each increase of around 12.5 km per week was associated with a marked rise in the odds of developing Achilles tendinopathy.
This reinforces a familiar but important principle: the Achilles tendon needs time to adapt to load. When running volume increases too quickly, or when weekly mileage remains high without adequate recovery, tendon remodelling may not keep pace with mechanical demand. For middle-aged and high-mileage runners in particular, monitoring training load is essential.
Therapists should therefore look beyond pain location and biomechanics alone. A careful training history remains central. Useful questions include:
How much has weekly mileage changed recently?
Has intensity, hill running, speed work or racing increased?
How many recovery days are included each week?
Has the runner recently changed footwear, terrain or training goals?
The study supports the view that Achilles tendinopathy prevention should begin with sensible load management, especially in runners accumulating higher weekly distances.
Foot strike may be less important than commonly assumed
One of the more clinically important findings is that footfall pattern was not significantly associated with future Achilles tendinopathy. In other words, rearfoot, midfoot or forefoot strike pattern did not clearly predict who developed the condition.
This challenges a common recommendation that runners should change foot strike to prevent Achilles problems. While foot strike can influence loading patterns, deliberately changing it may not be necessary and may even introduce new stresses if done abruptly.
For therapists, this means foot strike should not be treated as a universal correction target. A runner with Achilles pain does not automatically need to become a heel striker, midfoot striker or forefoot striker. Instead, gait changes should be individualised and linked to symptoms, load tolerance and functional goals.
Ankle rotation and inversion moment may matter
The study found two biomechanical variables that appeared to be protective: greater peak ankle external rotation and greater peak ankle inversion moment during the stance phase of running.
Reduced peak ankle external rotation was associated with higher odds of developing Achilles tendinopathy. A possible explanation is that some external foot rotation may help distribute force through the ankle–foot complex and reduce concentrated loading on the Achilles tendon. This does not mean therapists should simply tell all runners to “turn the foot out”. Rather, it suggests that excessively constrained or reduced transverse-plane movement may be relevant in some runners.
Greater peak ankle inversion moment was also associated with reduced odds of Achilles tendinopathy. This may reflect better frontal-plane ankle control and the ability to absorb and distribute load during stance. If inversion control is poor, the runner may rely more heavily on sagittal-plane loading through the calf–Achilles complex.
Clinically, this points toward the value of assessing ankle and foot control, not just calf strength. Therapists may consider including exercises that improve capacity and control in multiple planes, such as:
single-leg calf raises with good alignment;
controlled inversion and eversion strengthening;
single-leg balance and hopping progressions;
running drills that develop foot and ankle stiffness without excessive rigidity;
progressive plyometrics once symptoms and capacity allow.
The key is not to force a specific foot posture, but to build a more adaptable ankle–foot system.
Gait assessment should be individualised
The findings do not suggest that every runner needs high-tech gait analysis. However, they do support a more nuanced approach to movement assessment. Rather than focusing only on foot strike or visible pronation, therapists should consider how the whole lower limb manages load during stance.
A practical clinical gait assessment might include:
step rate and overstride;
ankle stiffness or excessive rigidity;
frontal-plane control at the foot, ankle, knee and hip;
calf endurance and fatigue response;
symmetry between limbs;
changes in mechanics at different speeds or when fatigued.
For runners with recurrent Achilles tendinopathy, especially high-mileage runners, more detailed gait assessment may help identify modifiable loading patterns.
Practical implications for therapy
This study supports a balanced approach to Achilles tendinopathy prevention and management. The most important clinical message is not that one running style is “good” and another is “bad”. Instead, risk appears to emerge from the interaction between load, tissue capacity and individual biomechanics.
For therapists, several practical principles follow.
First, monitor running volume carefully. Sudden increases in distance remain one of the most important warning signs.
Second, avoid overemphasising foot strike. There is currently no strong prospective evidence from this study that changing footfall pattern alone reduces Achilles tendinopathy risk.
Third, assess ankle–foot control in more than one plane. External rotation and inversion moment may reflect how effectively the lower limb distributes running loads.
Fourth, strengthen progressively. Rehabilitation should include calf strength, tendon loading, ankle control, balance and eventually running-specific plyometric capacity.
Finally, individualise advice. A gait change may help one runner but be unnecessary or counterproductive for another. Clinical reasoning should be based on symptoms, history, tissue capacity and movement behaviour, rather than generic rules about “ideal” running form.
Conclusion
Achilles tendinopathy in runners is best understood as a load-related condition influenced by individual biomechanics. This prospective study confirms that higher weekly running volume increases risk, while certain ankle mechanics during stance may be protective. Importantly, foot strike pattern alone did not predict injury.
For therapists, the message is clear: manage training load, build tendon and ankle capacity, and use gait assessment selectively and intelligently. The goal is not to create a perfect running style, but to help each runner develop enough strength, control and recovery capacity to tolerate the demands of running.
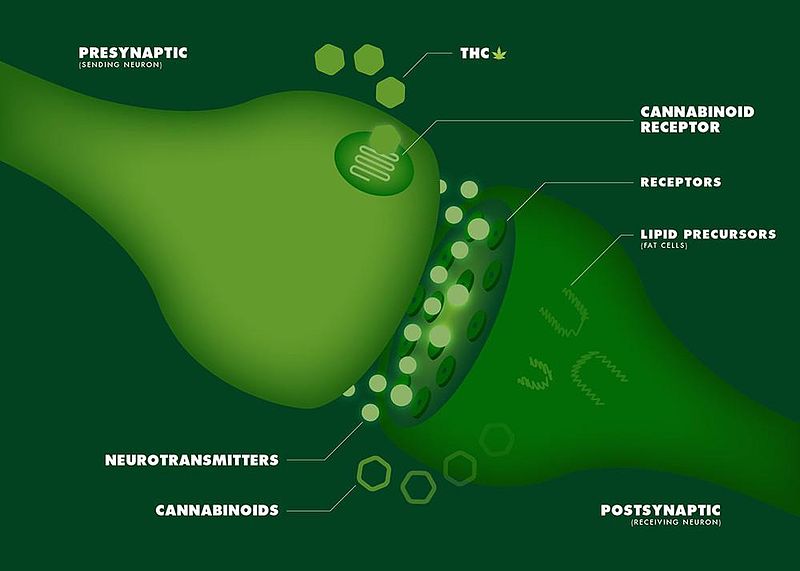
Expression of the endocannabinoid receptors in human fascial tissue
Evaluating the Clinical Impact of Myofascial Treatment: Physiological Changes vs. Patient-Centered Outcomes
